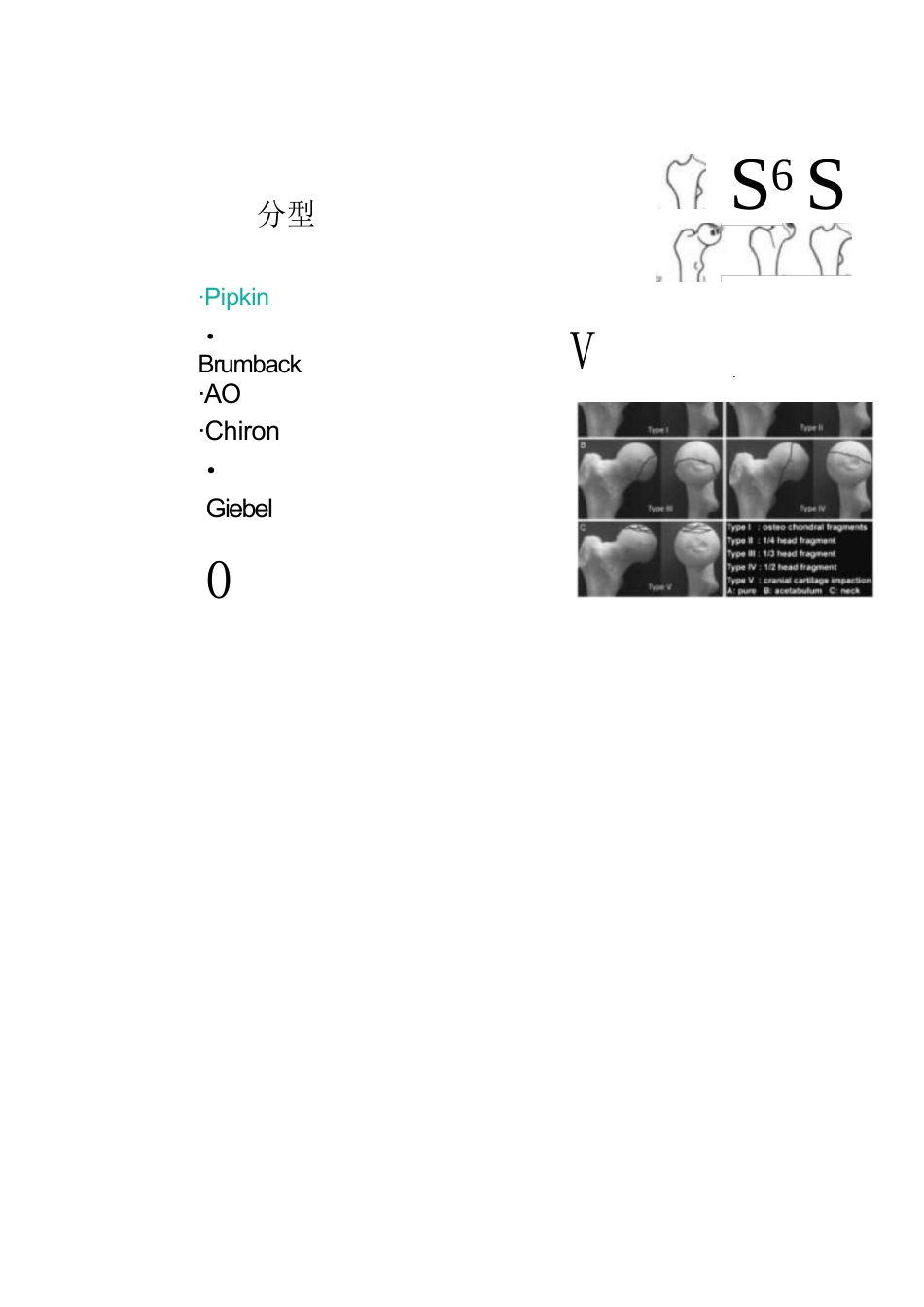
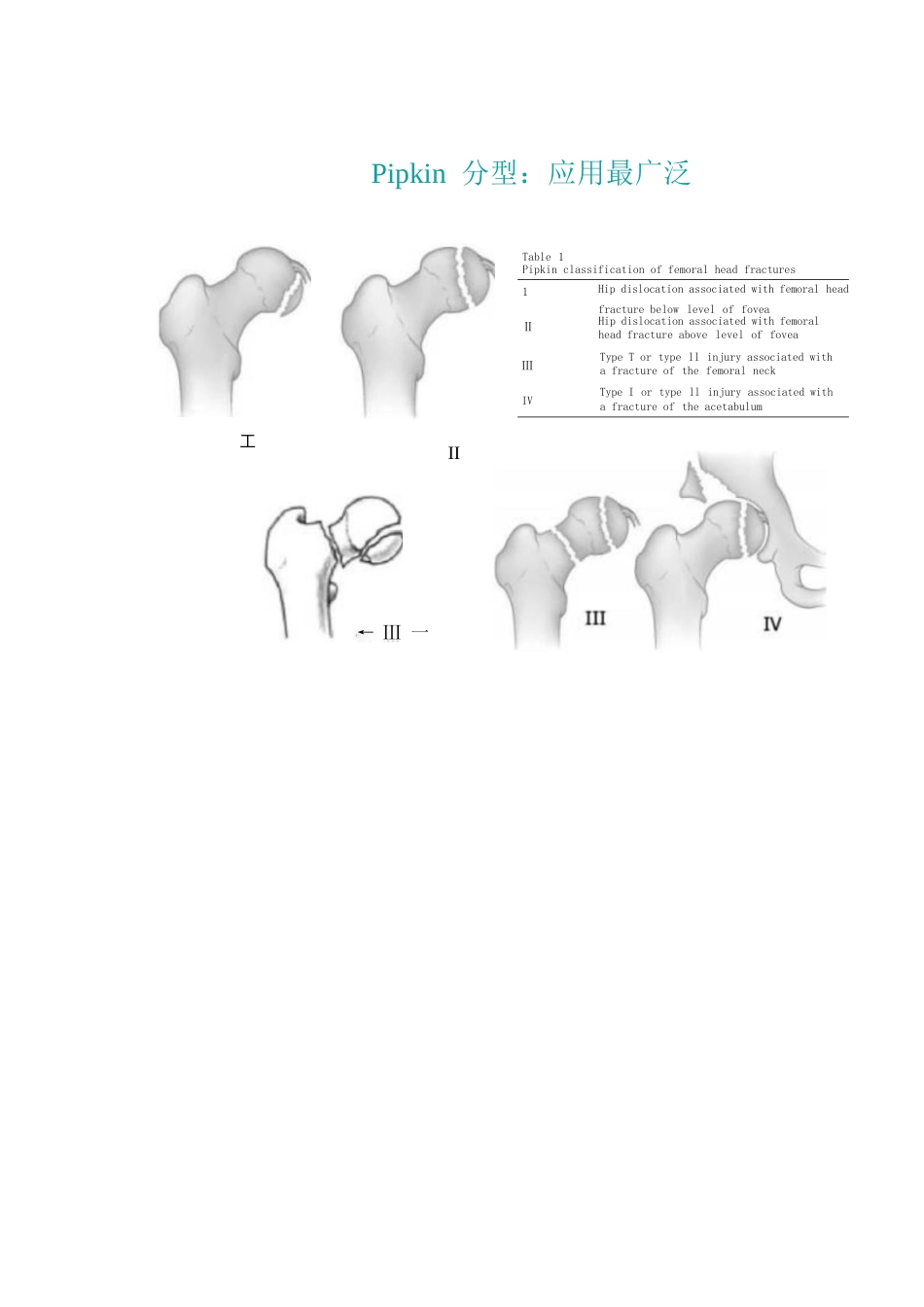
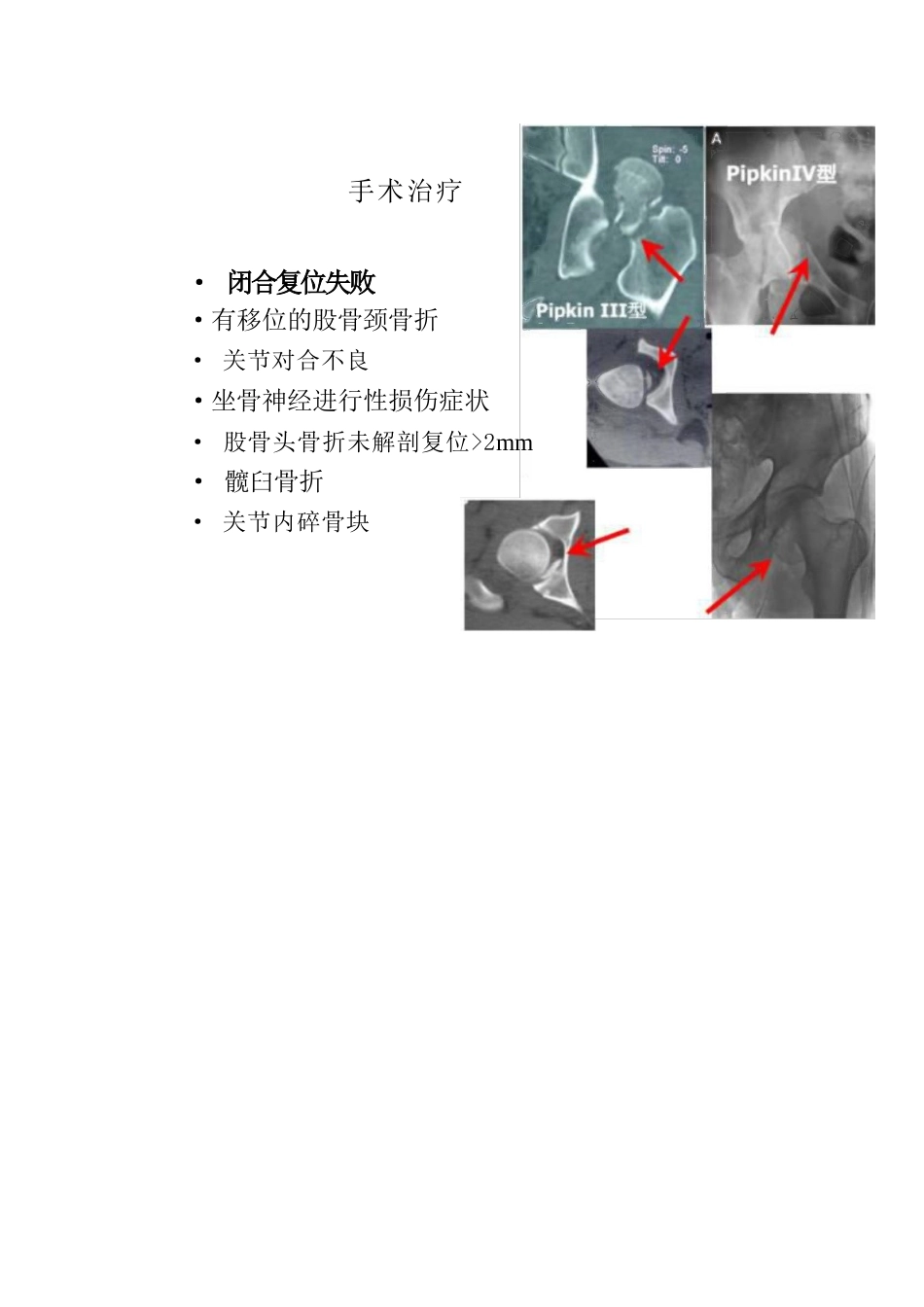
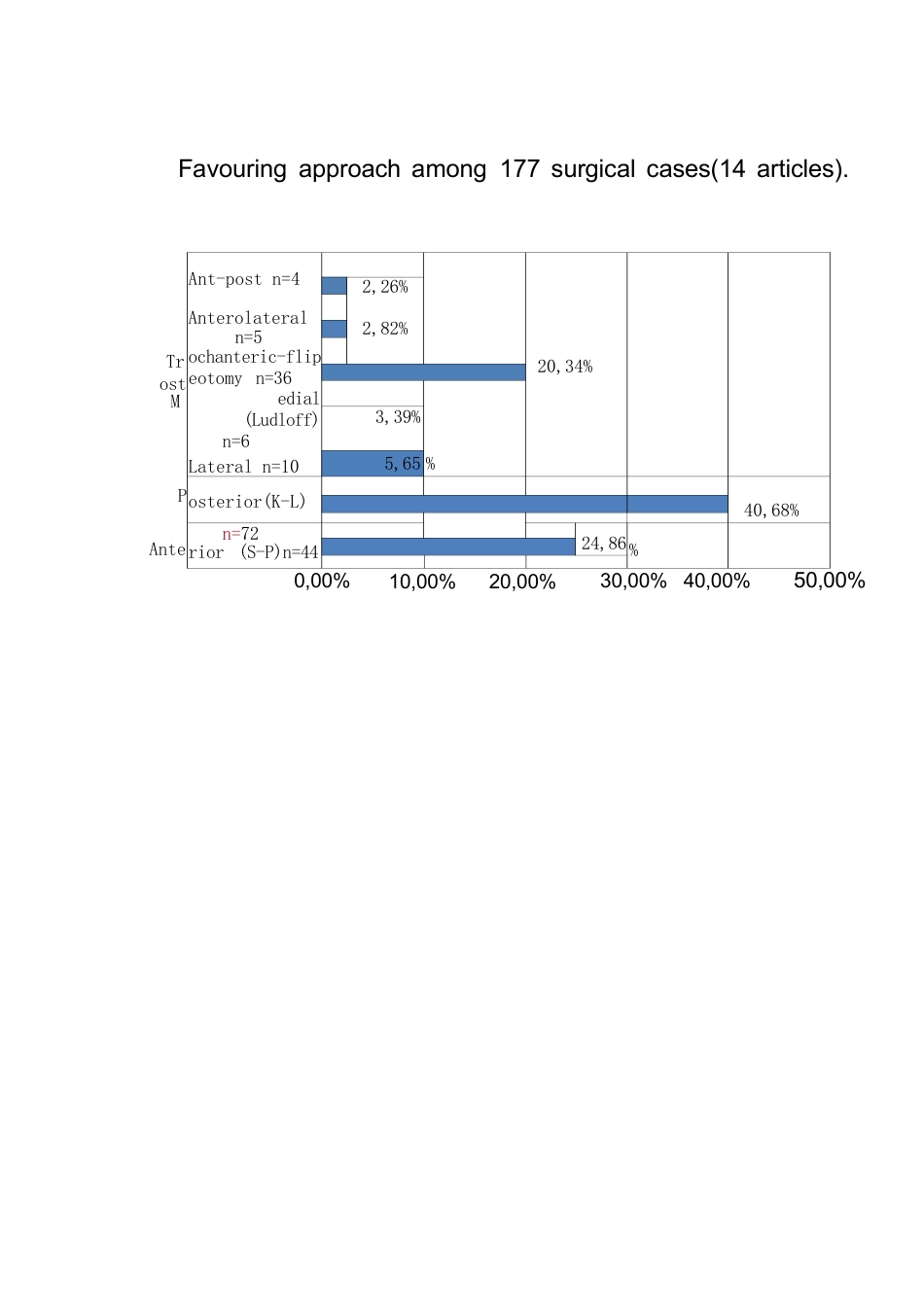
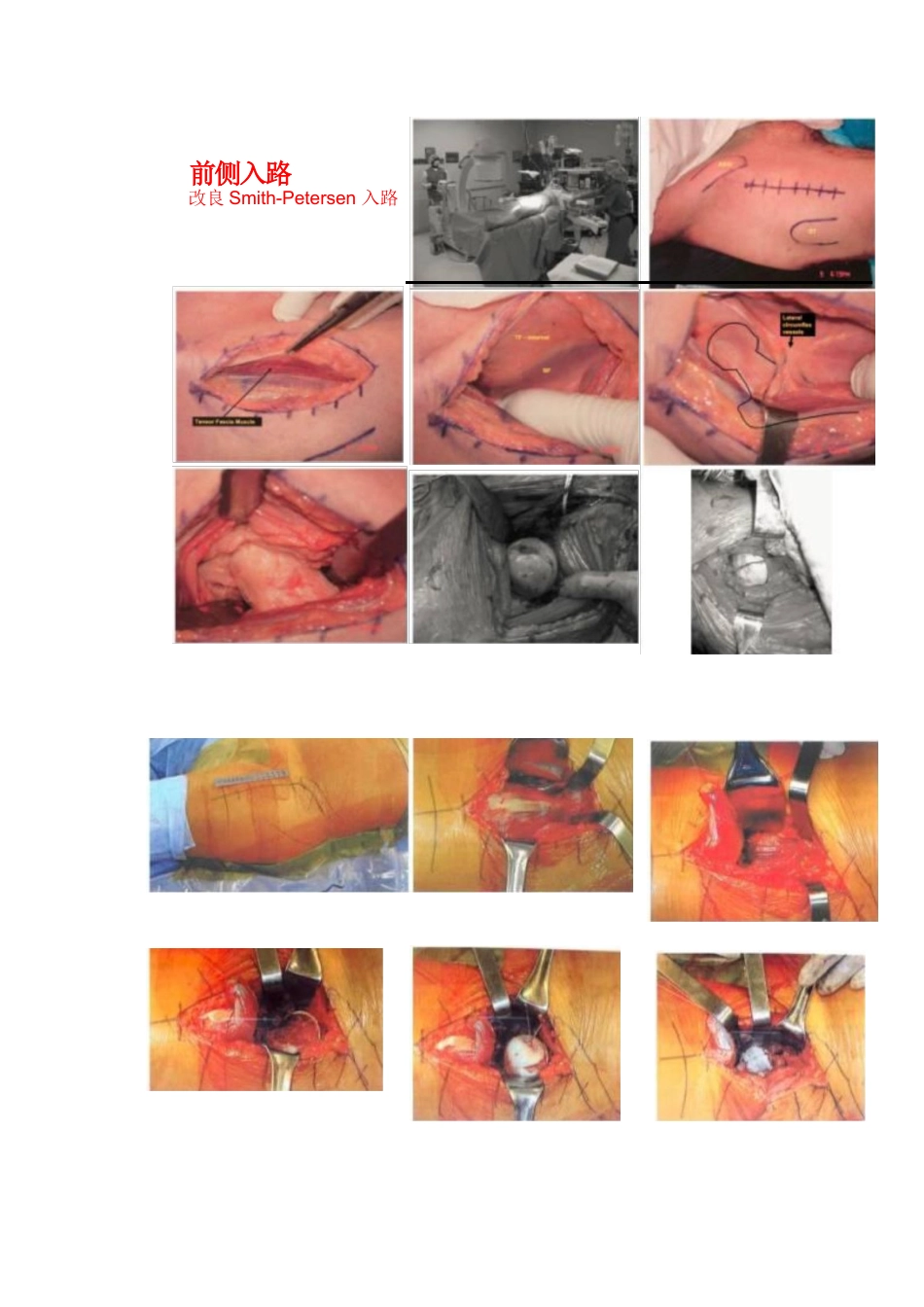
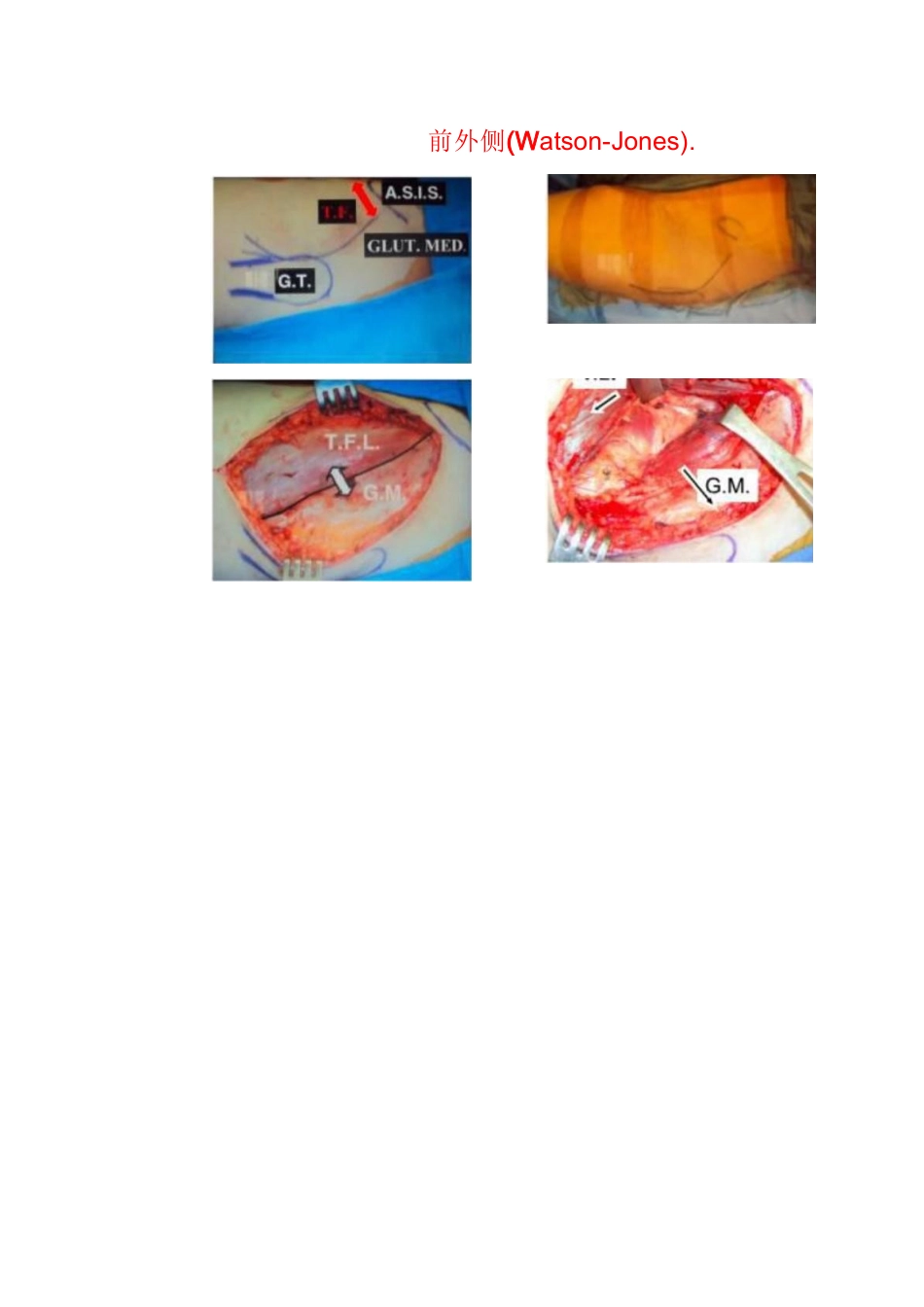
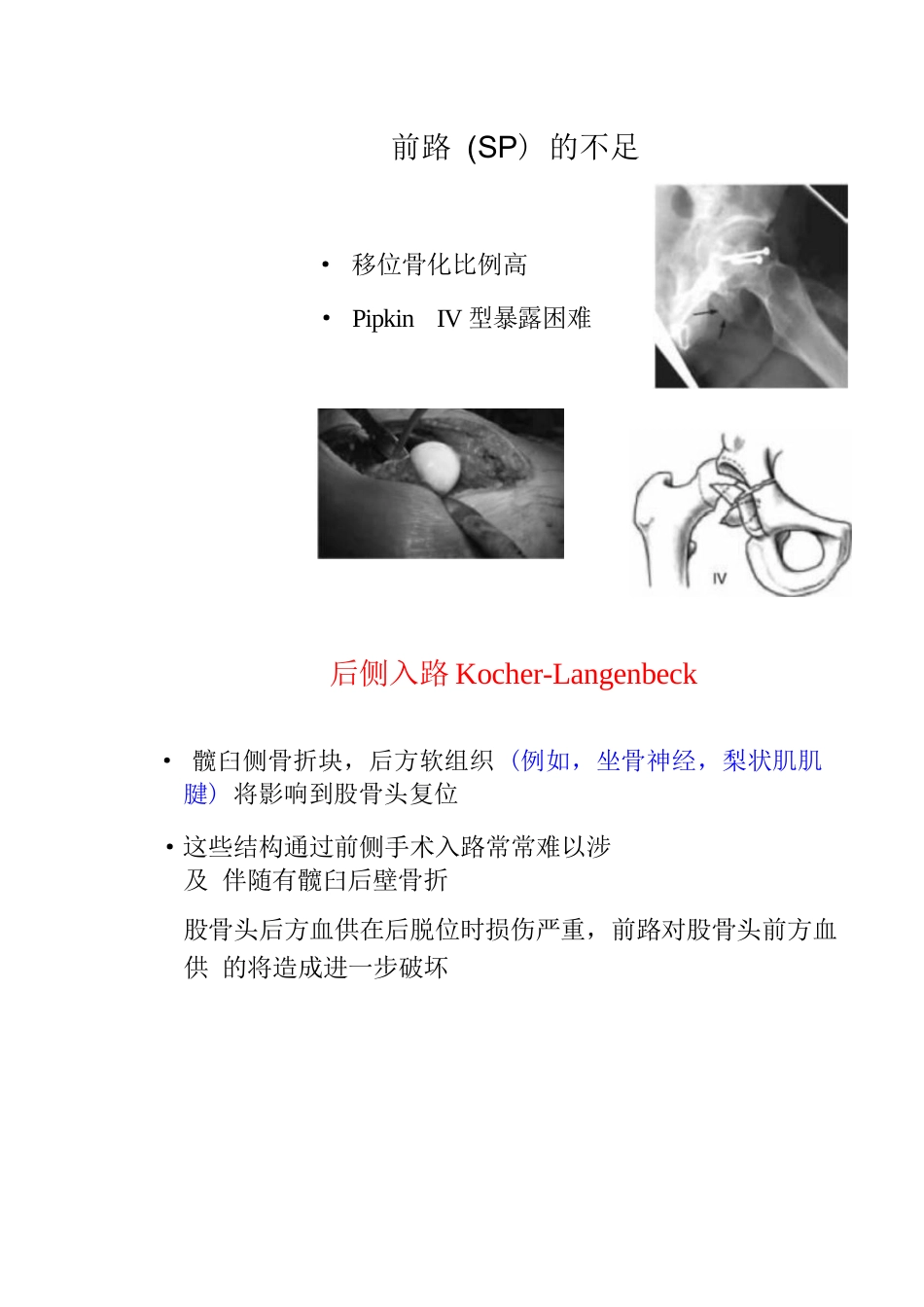
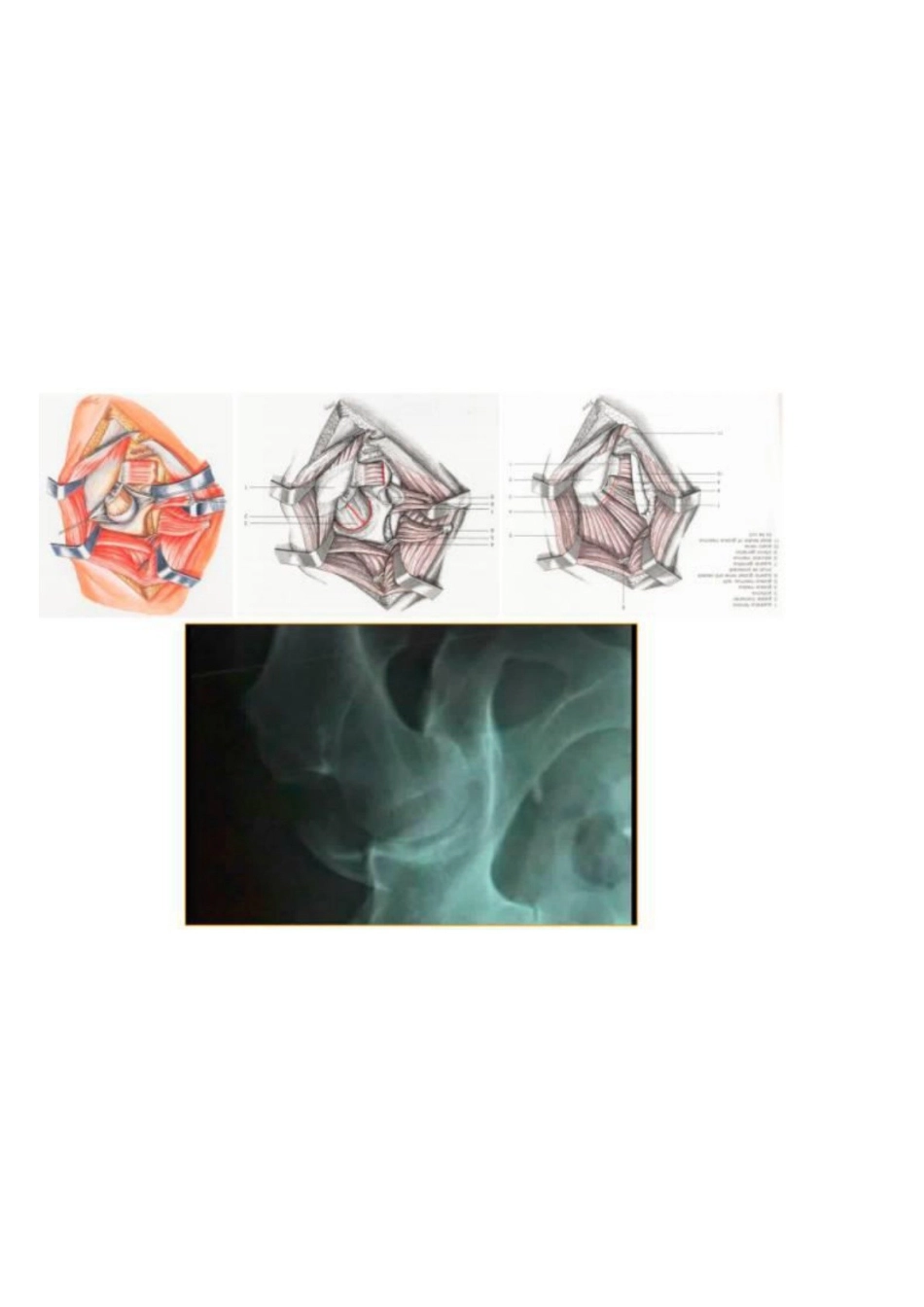
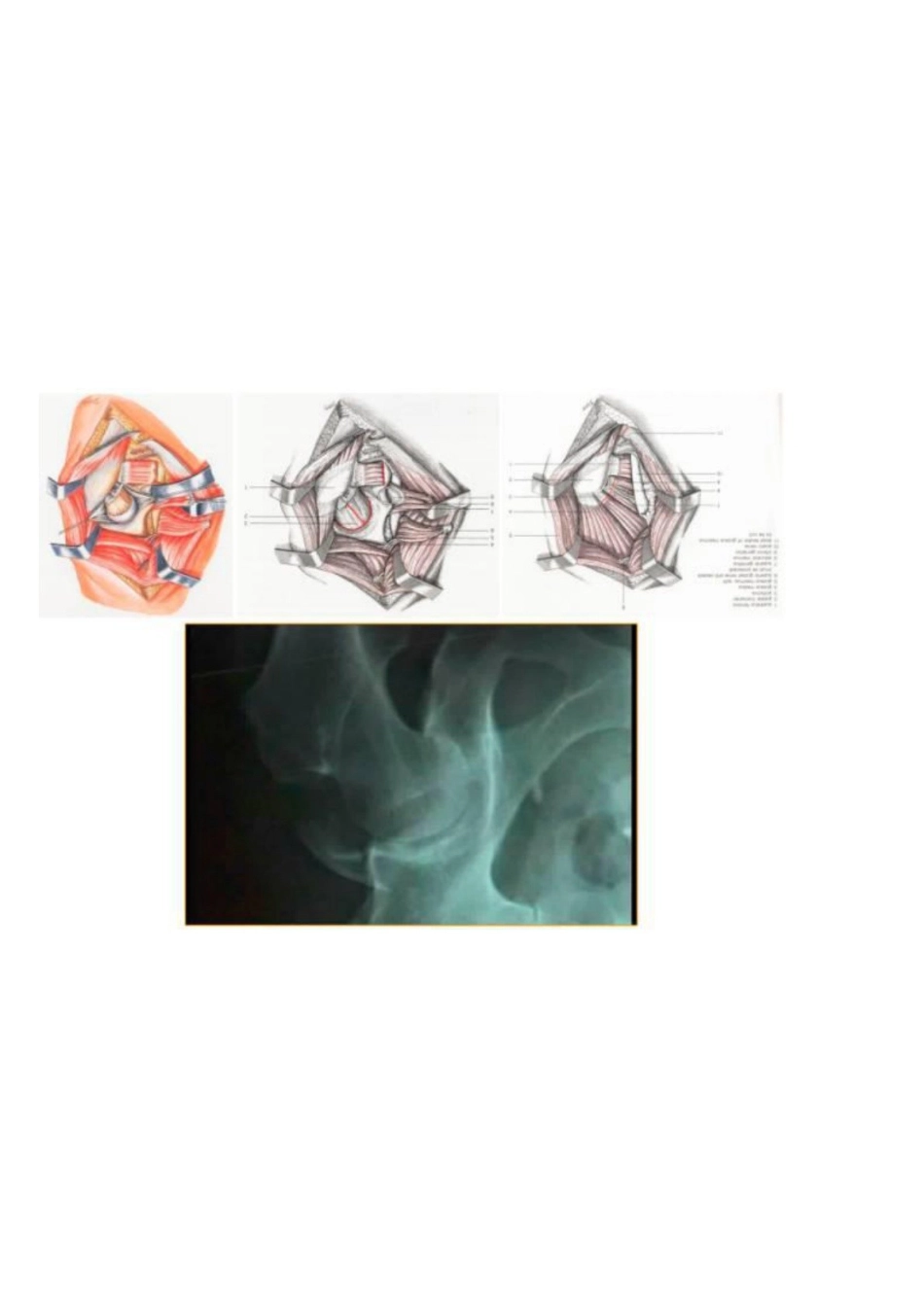
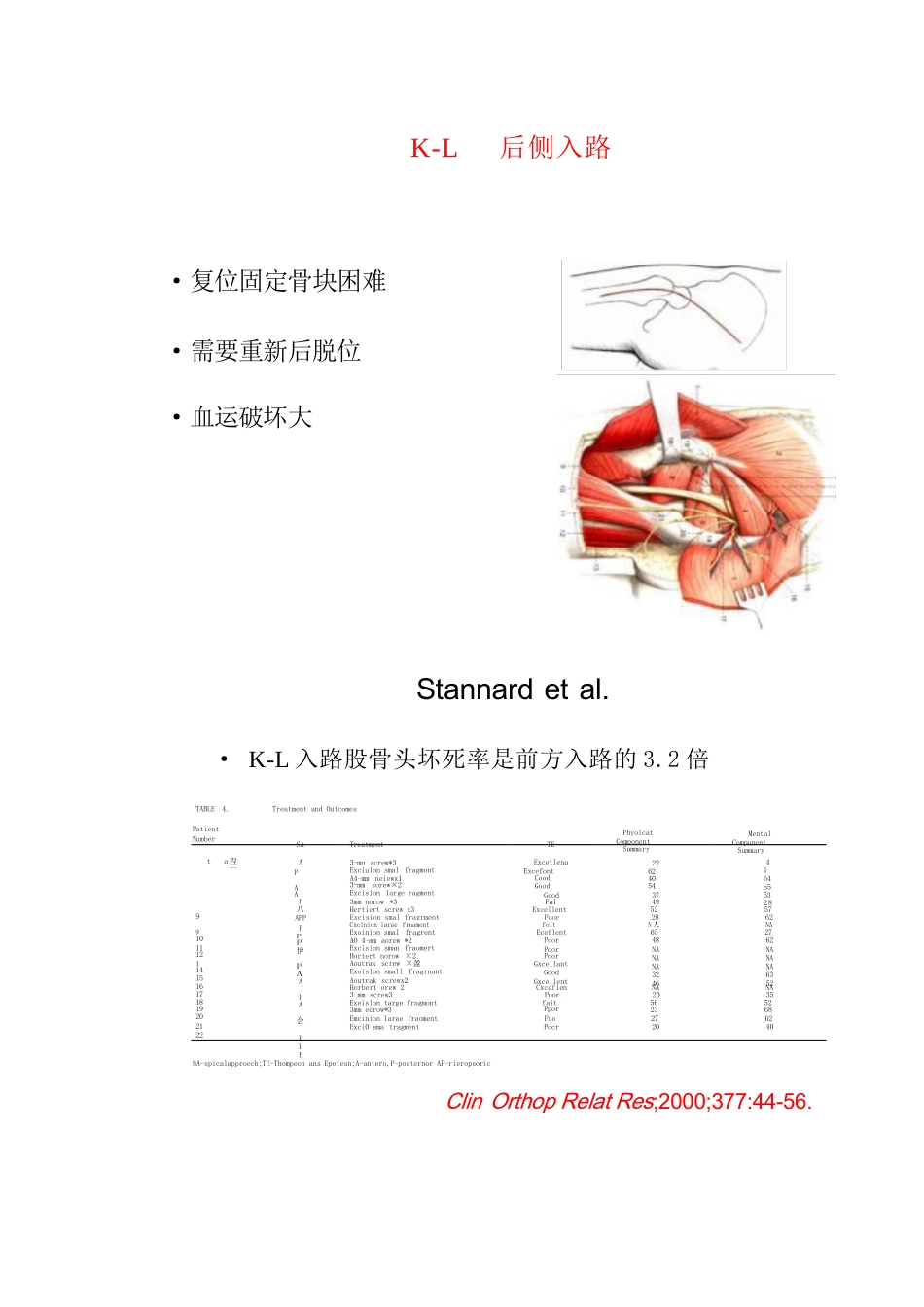
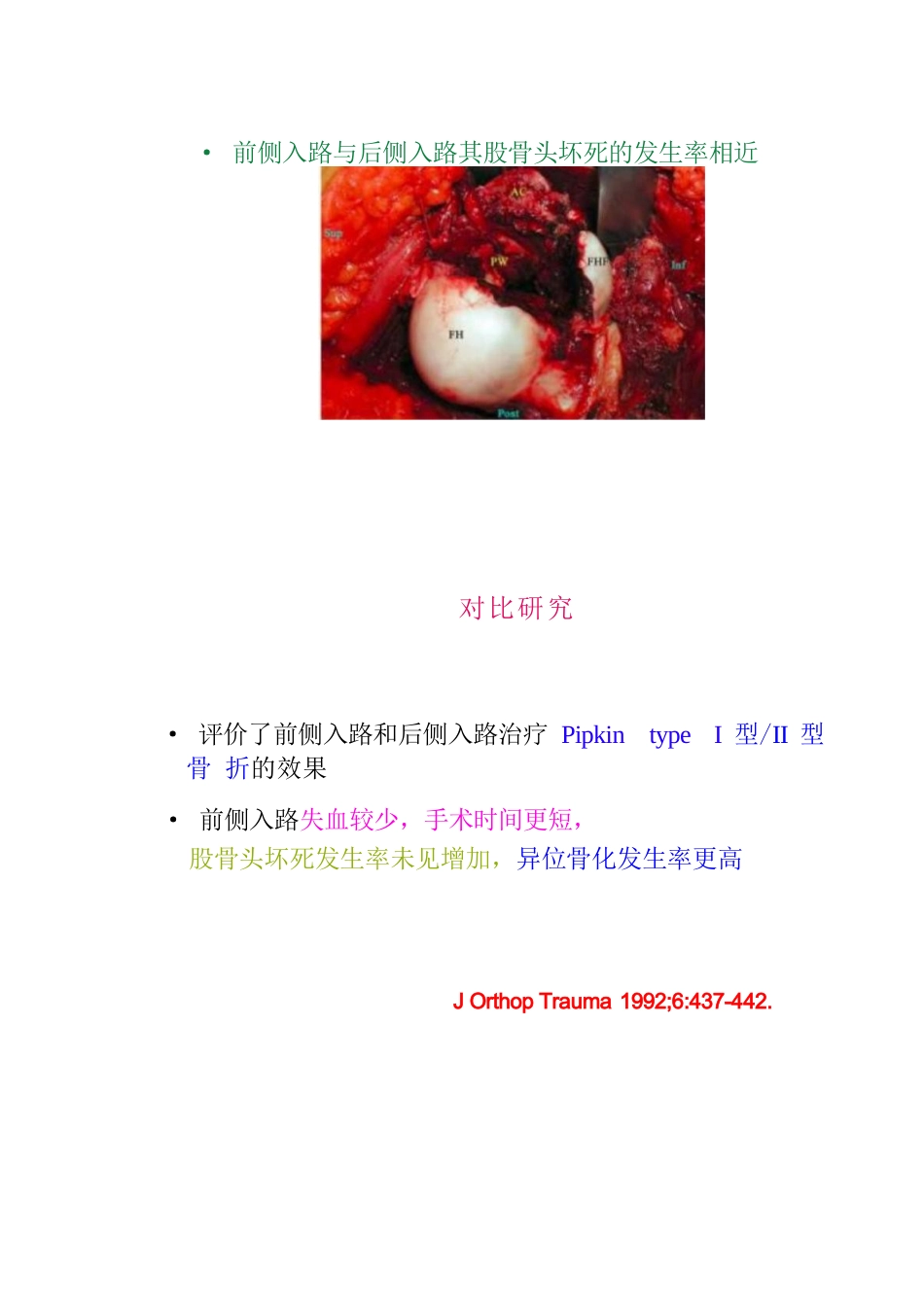
股骨头骨折DESCRIPT1ONDISLOCATION OP THE HEAD OF THEFEMUR,cOMPLICATED WITH IrsFBACTUBE;WITE KEMABK%.ar20 HLs 加HKET7, BCB,r09 anaLLe 血 -Lum,iBirke tt 1869年 首次描述分型·Pipkin· Brumback ·AO·Chiron· Giebel 0 S⁶SV.Pipkin 分型:应用最广泛Table 1Pipkin classification of femoral head fractures1Hip dislocation associated with femoral headⅡfracture below level of foveaHip dislocation associated with femoral head fracture above level of foveaⅢType T or type ll injury associated with a fracture of the femoral neckIVType I or type ll injury associated with a fracture of the acetabulum工II← Ⅲ 一手术治疗· 闭合复位失败·有移位的股骨颈骨折· 关节对合不良·坐骨神经进行性损伤症状· 股骨头骨折未解剖复位>2mm· 髋臼骨折· 关节内碎骨块手术入路· 内 侧 (Ludloff),· 后侧 (Kocher-Langenbeck), · 前 侧 (Smith-Petersen),· 外侧/前外侧 (Watson-Jones).Favouring approach among 177 surgical cases(14 articles).Ant-post n=4Anterolateral n=5ochanteric-flip eotomy n=36edial (Ludloff)n=6Lateral n=1020,34%2,26%2,82%%3,39%5,65osterior(K-L)40,68%n=72rior (S-P)n=4424,86%0,00% 10,00% 20,00% 30,00% 40,00% 50,00%TrostMAnteP前侧入路改良Smith-Petersen 入路前外侧(Watson-Jones).Smith-Petersen 入路·避免了对股骨头血供的额外损伤,并且比较容易显露股骨头骨 折块,股骨头骨折块通常在前内侧,通过后侧入路完成复位或 许比较困难前路( SP)· 时间短、出血少· 股骨头坏死率不增加· 便于复位和固定Swiontkowski(1992)Marchetti(1996)Stannard(2000)Kristensen (2002)前路 (SP) 的不足· 移位骨化比例高· Pipkin IV 型暴露困难后侧入路Kocher-Langenbeck· 髋臼侧骨折块,后方软组织 (例如,坐骨神经,梨状肌肌腱) 将影响到股骨头复位·这些结构通过前侧手术入路常常难以涉及 伴随有髋臼后壁骨折股骨头后方血供在后脱位时损伤严重,前路对股骨头前方血供 的将造成进一步破坏K-L 后侧入路·复位固定骨块困难·需要重新后脱位·血运破坏大Stannard et al.· K-L 入路股骨头坏死率是前方入路的3.2 倍TABLE 4. Treatment and Ou...